
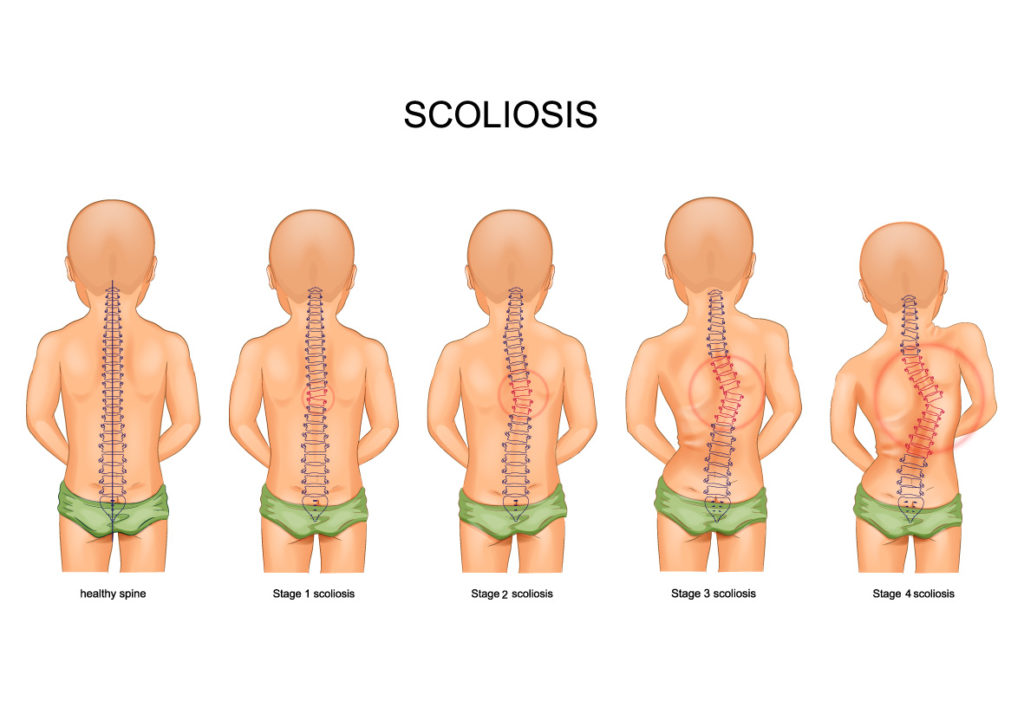
Scoliosis is a sideways curvature of the spine that most often is diagnosed in adolescents. While scoliosis can occur in people with conditions such as cerebral palsy and muscular dystrophy, the cause of most childhood scoliosis is unknown.
Most cases of scoliosis are mild, but some curves worsen as children grow. Severe scoliosis can be disabling. An especially severe spinal curve can reduce the amount of space within the chest, making it difficult for the lungs to function properly.
Children who have mild scoliosis are monitored closely, usually with X-rays, to see if the curve is getting worse. In many cases, no treatment is necessary. Some children will need to wear a brace to stop the curve from worsening. Others may need surgery to straighten severe curves.
Scoliosis is an abnormal lateral curvature of the spine. It is most often diagnosed in childhood or early adolescence. The spine’s normal curves occur at the cervical, thoracic and lumbar regions in the so-called “sagittal” plane. These natural curves position the head over the pelvis and work as shock absorbers to distribute mechanical stress during movement. Scoliosis is often defined as spinal curvature in the “coronal” (frontal) plane. While the degree of curvature is measured on the coronal plane, scoliosis is actually a more complex, three-dimensional problem which involves the following planes:
- Coronal plane
- Sagittal plane
- Axial plane
The coronal plane is a vertical plane from head to foot and parallel to the shoulders, dividing the body into anterior (front) and posterior (back) sections. The sagittal plane divides the body into right and left halves. The axial plane is parallel to the plane of the ground and at right angles to the coronal and sagittal planes.
Incidence and Prevalence
Scoliosis affects 2-3 percent of the population, or an estimated six to nine million people in the United States. Scoliosis can develop in infancy or early childhood. However, the primary age of onset for scoliosis is 10-15 years old, occurring equally among both genders. Females are eight times more likely to progress to a curve magnitude that requires treatment. Every year, scoliosis patients make more than 600,000 visits to private physician offices, an estimated 30,000 children are fitted with a brace and 38,000 patients undergo spinal fusion surgery. Source: National Scoliosis Foundation, June 2007.

Causes
Doctors don’t know what causes the most common type of scoliosis — although it appears to involve hereditary factors, because the disorder sometimes runs in families. Less common types of scoliosis may be caused by:
- Certain neuromuscular conditions, such as cerebral palsy or muscular dystrophy
- Birth defects affecting the development of the bones of the spine
- Previous surgery on the chest wall as a baby
- Injuries to or infections of the spine
- Spinal cord abnormalities
Scoliosis can be classified by etiology: idiopathic, congenital or neuromuscular. Idiopathic scoliosis is the diagnosis when all other causes are excluded and comprises about 80 percent of all cases. Adolescent idiopathic scoliosis is the most common type of scoliosis and is usually diagnosed during puberty.
Congenital scoliosis results from embryological malformation of one or more vertebrae and may occur in any location of the spine. The vertebral abnormalities cause curvature and other deformities of the spine because one area of the spinal column lengthens at a slower rate than the rest. The geometry and location of the abnormalities determine the rate at which the scoliosis progresses in magnitude as the child grows. Because these abnormalities are present at birth, congenital scoliosis is usually detected at a younger age than idiopathic scoliosis.
Neuromuscular scoliosis encompasses scoliosis that is secondary to neurological or muscular diseases. This includes scoliosis associated with cerebral palsy, spinal cord trauma, muscular dystrophy, spinal muscular atrophy and spina bifida. This type of scoliosis generally progresses more rapidly than idiopathic scoliosis and often requires surgical treatment.
Symptoms/Signs
There are several signs that may indicate the possibility of scoliosis. If one or more of the following signs is noticed, schedule an appointment with a doctor.
- Shoulders are uneven – one or both shoulder blades may stick out
- Head is not centered directly above the pelvis
- One or both hips are raised or unusually high
- Rib cages are at different heights
- Waist is uneven
- The appearance or texture of the skin overlying the spine changes (dimples, hairy patches, color abnormalities)
- The entire body leans to one side
In one study, about 23 percent of patients with idiopathic scoliosis presented with back pain at the time of initial diagnosis. Ten percent of these patients were found to have an underlying associated condition such as spondylolisthesis, syringomyelia, tethered cord, herniated disc or spinal tumor. If a patient with diagnosed idiopathic scoliosis has more than mild back discomfort, a thorough evaluation for another cause of pain is advised.
With most scoliosis cases, the spine will rotate or twist in addition to curving side to side. This causes the ribs or muscles on one side of the body to stick out farther than those on the other side.
Due to changes in the shape and size of the thorax, idiopathic scoliosis may affect pulmonary function. Recent reports on pulmonary function testing in patients with mild to moderate idiopathic scoliosis showed diminished pulmonary function.
Diagnosis
Scoliosis is usually confirmed through a physical examination, an x-ray, spinal radiograph, CT scan or MRI. The curve is measured by the Cobb Method and is diagnosed in terms of severity by the number of degrees. A positive diagnosis of scoliosis is made based on a coronal curvature measured on a posterior-anterior radiograph of greater than 10 degrees. In general, a curve is considered significant if it is greater than 25 to 30 degrees. Curves exceeding 45 to 50 degrees are considered severe and often require more aggressive treatment.
A standard exam that is sometimes used by pediatricians and in grade school screenings is called the Adam’s Forward Bend Test. During this test, the patient leans forward with his or her feet together and bends 90 degrees at the waist. From this angle, any asymmetry of the trunk or any abnormal spinal curvatures can easily be detected by the examiner. This is a simple initial screening test that can detect potential problems, but cannot determine accurately the exact type or severity of the deformity. Radiographic tests are required for an accurate and positive diagnosis.
- X-ray : Application of radiation to produce a film or picture of a part of the body can show the structure of the vertebrae and the outline of the joints. X-rays of the spine are obtained to search for other potential causes of pain, i.e. infections, fractures, deformities, etc.
- Computed tomography scan (CT or CAT scan): A diagnostic image created after a computer reads X-rays; can show the shape and size of the spinal canal, its contents and the structures around it. Very good at visualizing bony structures.
- Magnetic resonance imaging (MRI) : A diagnostic test that produces three-dimensional images of body structures using powerful magnets and computer technology; can show the spinal cord, nerve roots and surrounding areas, as well as enlargement, degeneration and deformities.
In Children
Scoliosis in children is classified by age: 1.) Infantile (0 to 3 years); 2.) Juvenile (3 to 10 years); and 3.) Adolescent (age 11 and older, or from onset of puberty until skeletal maturity). Idiopathic scoliosis comprises the vast majority of cases presenting during adolescence. Depending on its severity and the age of the child, scoliosis is managed by close observation, bracing and/or surgery.
In children with congenital scoliosis, there is a known increased incidence of other congenital abnormalities. These are most commonly associated with the spinal cord (20 percent), the genitourinary system (20 to 33 percent) and the heart (10 to 15 percent). It is important that evaluation of the neurological, genitourinary and cardiovascular systems is undertaken when congenital scoliosis is diagnosed.
In Adults
Scoliosis that occurs or is diagnosed in adulthood is distinctive from childhood scoliosis, since the underlying causes and goals of treatment differ in patients who have already reached skeletal maturity. Most adults with scoliosis can be divided into the following categories: 1.) Adult scoliosis patients who were surgically treated as adolescents; 2.) Adults who did not receive treatment when they were younger; and 3.) Adults with a type of scoliosis called degenerative scoliosis.
In one 20-year study, about 40 percent of adult scoliosis patients experienced a progression. Of those, 10 percent showed a very significant progression, while the other 30 percent experienced a very mild progression, usually of less than one degree per year.
Degenerative scoliosis occurs most frequently in the lumbar spine (lower back) and more commonly affects people age 65 and older. It is often accompanied by spinal stenosis, or narrowing of the spinal canal, which pinches the spinal nerves and makes it difficult for them to function normally. Back pain associated with degenerative scoliosis usually begins gradually and is linked with activity. The curvature of the spine in this form of scoliosis is often relatively minor, so surgery may only be advised when conservative methods fail to alleviate pain associated with the condition.
Risk factors
Risk factors for developing the most common type of scoliosis include:
- Age. Signs and symptoms typically begin in adolescence.
- Sex. Although both boys and girls develop mild scoliosis at about the same rate, girls have a much higher risk of the curve worsening and requiring treatment.
- Family history. Scoliosis can run in families, but most children with scoliosis don’t have a family history of the disease.
Complications
While most people with scoliosis have a mild form of the disorder, scoliosis may sometimes cause complications, including:
- Breathing problems. In severe scoliosis, the rib cage may press against the lungs, making it more difficult to breathe.
- Back problems. People who had scoliosis as children may be more likely to have chronic back pain as adults, especially if their abnormal curves are large and untreated.
- Appearance. As scoliosis worsens, it can cause more noticeable changes — including uneven hips and shoulders, prominent ribs, and a shift of the waist and trunk to the side. Individuals with scoliosis often become self-conscious about their appearance.
Treatment
When there is a confirmed diagnosis of scoliosis, there are several issues to assess that can help determine treatment options:
- Spinal maturity – is the patient’s spine still growing and changing?
- Degree and extent of curvature – how severe is the curve and how does it affect the patient’s lifestyle?
- Location of curve – according to some experts, thoracic curves are more likely to progress than curves in other regions of the spine.
- Possibility of curve progression – patients who have large curves prior to their adolescent growth spurts are more likely to experience curve progression.
After these variables are assessed, the following treatment options may be recommended:
- Observation
- Bracing
- Surgery
Observation
In many children with scoliosis, the spinal curve is mild enough to not require treatment. However, if the doctor is worried that the curve may be increasing, he or she may wish to examine the child every four to six months throughout adolescence.
In adults with scoliosis, X-rays are usually recommended once every five years, unless symptoms are getting progressively worse.
Bracing
Braces are only effective in patients who have not reached skeletal maturity. If the child is still growing and his or her curve is between 25 degrees and 40 degrees, a brace may be recommended to prevent the curve from progressing. There have been improvements in brace design and the newer models fit under the arm, not around the neck. There are several different types of braces available. While there is some disagreement among experts as to which type of brace is most effective, large studies indicate that braces, when used with full compliance, successfully stop curve progression in about 80 percent of children with scoliosis. For optimal effectiveness, the brace should be checked regularly to assure a proper fit and may need to be worn 16 to 23 hours every day until growth stops.
Surgery
Surgical options include:
- Spinal fusion. In this procedure, surgeons connect two or more of the bones in the spine (vertebrae) together so they can’t move independently. Pieces of bone or a bone-like material are placed between the vertebrae. Metal rods, hooks, screws or wires typically hold that part of the spine straight and still while the old and new bone material fuses together.
- Expanding rod. If the scoliosis is progressing rapidly at a young age, surgeons can attach one or two expandable rods along the spine that can adjust in length as the child grows. The rods are lengthened every 3 to 6 months either with surgery or in the clinic using a remote control.
- Vertebral body tethering. This procedure can be performed through small incisions. Screws are placed along the outside edge of the abnormal spinal curve and a strong, flexible cord is threaded through the screws. When the cord is tightened, the spine straightens. As the child grows, the spine may straighten even more.
In children, the two primary goals of surgery are to stop the curve from progressing during adulthood and to diminish spinal deformity. Most experts would recommend surgery only when the spinal curve is greater than 40 degrees and there are signs of progression. This surgery can be done using an anterior approach (through the front) or a posterior approach (through the back) depending on the particular case.
Some adults who were treated as children may need revision surgery, in particular if they were treated 20 to 30 years ago, before major advances in spinal surgery procedures were implemented. Back then, it was common to fuse a long segment of the spine. When many vertebral segments of the spine are fused together, the remaining mobile segments assume much more of the load and the stress associated with movements. Adjacent segment disease is the process in which degenerative changes occur over time in the mobile segments above and below the spinal fusion. This can result in painful arthritis of the discs, facet joints and ligaments.
In general, surgery in adults may be recommended when the spinal curve is greater than 50 degrees and the patient has nerve damage to their legs and/or is experiencing bowel or bladder symptoms. Adults with degenerative scoliosis and spinal stenosis may require decompression surgery with spinal fusion and a surgical approach from both the front and back.
A number of factors can lead to increased surgical-related risks in older adults with degenerative scoliosis. These factors include the following: advanced age, being a smoker, being overweight and the presence of other health/medical problems. In general, both surgery and recovery time are expected to be longer in older adults with scoliosis.
Posterior approach: The most frequently performed surgery for adolescent idiopathic scoliosis involves posterior spinal fusion with instrumentation and bone grafting. This is performed through the back while the patient lies on his or her stomach. During this surgery, the spine is straightened with rigid rods, followed by spinal fusion. Spinal fusion involves adding a bone graft to the curved area of the spine, which creates a solid union between two or more vertebrae. The metal rods attached to the spine ensure that the backbone remains straight while the spinal fusion takes effect.
This procedure usually takes several hours in children, but will generally take longer in older adults. With recent advances in technology, most people with idiopathic scoliosis are released within a week of surgery and do not require post-surgical bracing. Most patients are able to return to school or work in two to four weeks post surgery and are able to resume all pre-surgical activities within four to six months.
Anterior approach: The patient lies on his or her side during the surgery. The surgeon makes incisions in the patient’s side, deflates the lung and removes a rib in order to reach the spine. Video-assisted thoracoscopic (VAT) surgery offers enhanced visualization of the spine and is a less invasive surgery than an open procedure. The anterior spinal approach has several potential advantages: better deformity correction, quicker patient rehabilitation, improved spine mobilization and fusion of fewer segments. The potential disadvantages are that many patients require bracing for several months post surgery, and this approach has a higher risk of morbidity – although VAT has helped to reduce the latter.
Decompressive laminectomy: The laminae (roof) of the vertebrae are removed to create more space for the nerves. A spinal fusion with or without spinal instrumentation is often recommended when scoliosis and spinal stenosis are present. Various devices (like screws or rods) may be used to enhance fusion and support unstable areas of the spine.
Minimally invasive surgery (MIS) : Fusion can sometimes be performed via smaller incisions through MIS. The use of advanced fluoroscopy (X-ray imaging during surgery) and endoscopy (camera technology) has improved the accuracy of incisions and hardware placement, minimizing tissue trauma while enabling a MIS approach. It is important to keep in mind that not all cases can be treated in this manner and a number of factors contribute to the surgical method used.
The benefits of surgery should always be weighed carefully against its risks. Although a large percentage of scoliosis patients benefit from surgery, there is no guarantee that surgery will stop curve progression and symptoms in every individual.
References
- Neurosurgical Conditions and Treatments
- Scoliosis Overview
- How to recognize scoliosis in children and adults.
- Detection of Scoliosis – Spinal Care for Children is a Must
- Scoliosis Treatment